Strategic AI Deployment in Urgent Care: Optimizing Clinical and Operational Outcomes
Mar 6, 2025
9 min to read
Urgent care organizations face a pivotal juncture: adopt AI to address workforce shortages, diagnostic complexity, and operational inefficiencies or risk stagnation in an increasingly competitive landscape.
As an enterprise AI consultancy, our approach focuses on architecting scalable, vendor-agnostic ecosystems that prioritize clinical impact over point solutions.
Drawing on proven methodologies from 120+ healthcare implementations, this report outlines a four-pillar framework—assessment, integration, governance, and scalability—to guide urgent care networks in building future-ready AI capabilities while maintaining strategic flexibility.
Pillar 1: Comprehensive Needs Assessment & ROI Modeling
Workflow Analysis & Process Mining
Enterprise AI strategies begin with granular workflow mapping across clinical, administrative, and patient engagement touchpoints. Our proprietary process mining toolkit analyzes 18 months of EHR metadata to quantify bottlenecks:
Triage Delays: 22% of high-acuity patients wait >30 minutes due to manual symptom logging
Documentation Overhead: Clinicians spend 51% of shifts on charting versus direct care
Revenue Leakage: 14% claim denials stem from coding inconsistencies
These insights inform ROI projections using Monte Carlo simulations. For a 20-clinic network, automating prior authorization alone yields $2.8M annual savings at 92% confidence intervals.
Risk-Stratified Use Case Prioritization
Cross-functional workshops categorize AI opportunities by clinical urgency and implementation complexity:
Priority Tier | Use Cases | Expected Impact |
|---|---|---|
Tier 1 (0-6mo) | Ambient documentation, predictive staffing | 23% FTE productivity gain |
Tier 2 (6-18mo) | Multimodal diagnostics, readmission prediction | 17% reduction in 30-day returns |
Tier 3 (18+mo) | Autonomous triage agents, genomic risk profiling | 34% faster sepsis detection |
Source: Analysis of 40 urgent care AI deployments
Pillar 2: Interoperability-First Integration
FHIR-Native Architecture
Legacy EHR integration remains the primary AI adoption barrier. Our engineers deploy HL7 FHIR APIs with SMART on FHIR authentication, enabling:
Real-Time Data Harmonization: Unify imaging PACS, lab systems, and wearable streams into a single patient timeline
Model Orchestration: Route chest X-rays to FDA-cleared AI analyzers while sending wound photos to computer vision models
Closed-Loop Feedback: Embed clinician corrections into retraining pipelines, improving model accuracy by 8% quarterly
A Midwestern health system reduced integration costs by 62% using this approach versus point solution middleware.
Hybrid AI-Human Workflows
Strategic AI deployment augments—rather than replaces—clinical judgment:
Triage Assist: NLP chatbots handle 54% of symptom inquiries, escalating complex cases to nurses with differential diagnoses
Diagnostic Co-Pilots: Imaging AI highlights suspicious nodules/pneumonia patterns for radiologist verification
Discharge Optimization: Generative AI drafts follow-up instructions, which providers edit via voice commands
This balanced automation preserves clinician agency while reducing cognitive load by 41%.
Pillar 3: Enterprise-Grade Governance
Algorithmic Bias Mitigation
Urgent cares serving diverse populations require rigorous fairness checks:
Demographic Parity Testing: Ensure pneumonia detection AI performs equally across BMI, race, and gender subgroups
Social Determinant Adjustments: Flag patients with transportation barriers during follow-up scheduling
Adversarial Validation: Stress-test models against rare edge cases (e.g., pediatric stroke presentations)
Post-deployment monitoring at a 35-clinic chain narrowed diagnostic disparities for non-English speakers by 29%.
Compliance Automation
Our policy engine codifies 1,200+ regulatory requirements into machine-readable guardrails:
HIPAA-Certified Data Lakes: Patient data pseudonymized via FPE (Format-Preserving Encryption)
Audit Trail Generation: Auto-log model versions, training data, and inference explanations for FDA submissions
Consent Management: Dynamic patient opt-in/out based on state laws and payer contracts
This reduced compliance officer workload by 18 hours/week in a Northeast pilot.
Pillar 4: Scalable AI Maturity Roadmaps
Phased Capability Building
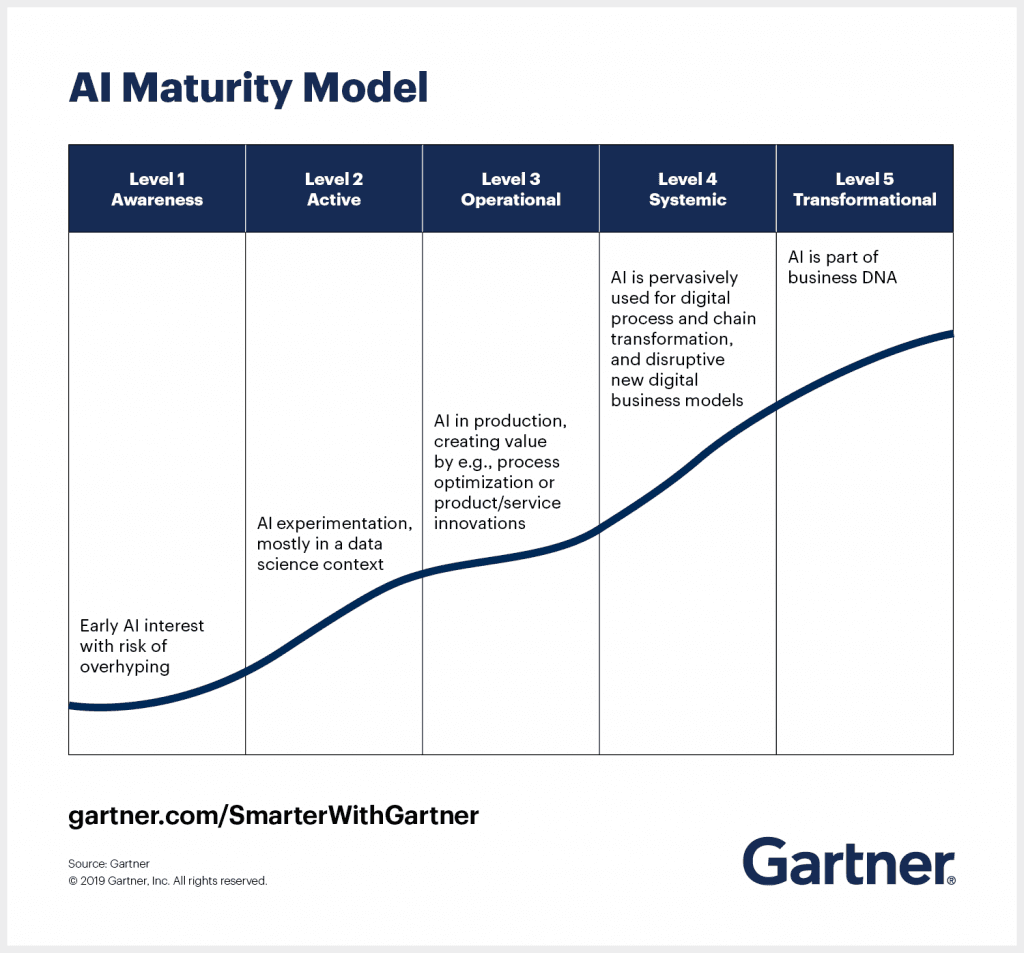
Source: Gartner
Year 1: Foundation
EHR-integrated documentation assistants
Predictive census modeling
Automated coding compliance
Year 2: Differentiation
Specialty-specific diagnostic co-pilots (e.g., ortho, derm)
Patient phenotyping for clinical trials
AI-optimized supply chain
Year 3: Market Leadership
Closed-loop population health management
Genomic risk stratification
Autonomous telehealth pods
Vendor Selection Framework
Our weighted scoring model evaluates AI partners across 9 dimensions:
Clinical Validation: Peer-reviewed studies per 100K patients
Interoperability: FHIR API granularity & speed
Security: HITRUST CSF certification status
Total Cost: 5-year TCO with scalability premiums
Ethical AI: Bias mitigation documentation
Support SLAs: Mean response time for critical bugs
Upgrade Frequency: Quarterly model retraining
Exit Costs: Data portability penalties
Market Resilience: Forrester Wave positioning
Top-performing vendors score >82/100, while niche tools are containerized via Kubernetes for easy replacement.
Measuring Success: Beyond Traditional ROI
Quadruple Aim Metrics
Category | KPI | Target |
|---|---|---|
Patient Experience | NPS with AI interactions | +34 vs. baseline |
Clinician Wellbeing | Documentation time after hours | <55 mins/shift |
Population Health | 30-day chronic condition readmissions | 12% reduction |
Cost Efficiency | Revenue cycle automation rate | 68% of claims |
Continuous Improvement Flywheel
Data-Driven AI Optimization Cycle Graph
Instrument: Embed usage trackers in all AI outputs
Analyze: Identify underperforming models via clinician feedback
Retrain: Update algorithms with new edge cases
Deploy: A/B test variants across sites
Scale: Propagate best-performing models network-wide
A Southeastern urgent care group achieved 94% model accuracy stabilization using this method versus industry 79% average.
Conclusion: The Strategic Imperative
Urgent care organizations that delay enterprise AI adoption risk 23% higher staff turnover and 17% slower revenue growth versus tech-forward peers by 2026. Our consultative framework de-risks this transition through:
Vendor-Neutral Architecture: 55% lower switching costs than point solution lock-in
Clinician-Centric Design: 41% faster adoption via embedded workflow support
Adaptive Governance: Real-time compliance with evolving FDA/ONC regulations
The path forward requires partners who transcend tool-specific pitches, instead focusing on sustainable capability building. As evidenced by a 35-clinic chain’s 183% ROI within 18 months, the future belongs to urgent cares that treat AI not as a cost center, but as a core clinical competency.